

The 400 patients of ureteric stone during the period of January 2000 – June 2009 were included in this prospective the study.
In this study 240 patients were male as compared to female 140 female patients. Age of the patients varies between 17-58 years with average age being 26.5 years. Most common presentation in this study was ureteric colic (70%) followed by burning micturition (50%) followed by vomiting (40%) and fixed renal pain in 30% cases. Most common sign was haematuria (80%).
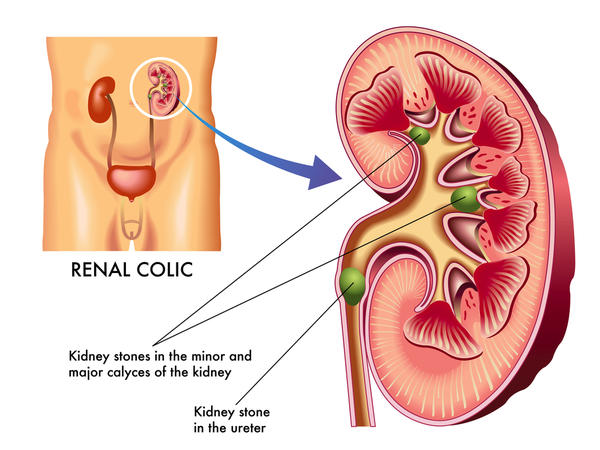
A stone in the ureter usually arises in the kidney and enters in to the ureter subsequently. Most calculi are small and pass spontaneously. Typically most patients present with sudden onset of agonizing pain, which may radiate to the groin, sacrum, labia, scrotum and the anterior surface of thigh. Presence of stone in ureter does not necessitate the surgical intervention.
Important factors that decide spontaneous passage of stones are its size, location and degree of obstruction at the initial presentation. Conservative treatment or medical treatment is probably most effective for stone size of 3- 10mm.
Overall incidence of stone passage with medical treatment is >65%. Many randomized trials prove the efficacy of conservative or medical treatment and helps in reducing the pain and helps in stone passage. Thus overall rate of surgical intervention is reduced with medical treatment. Conservative treatment using medical therapy is found to be cost-effective before embarking upon surgical option.
Most stone that will pass spontaneously with conservative management, will pass within 4-6 weeks. According to meta-analysis done by Marlene Busko conclude that all patients with stone size up to 1 cm who are candidate for observation should be offered trial of medical therapy. Conservative or medical management should not be offered to patients with >1cm size stone, high grade obstruction or patients in sepsis.
According to Pak et al, high fluid intake in such ways that urine output remains above 3 liters per day, has shown that there is reduction in saturation of calcium phosphate, calcium oxalate thus decreasing the chances of stone formation. High fluid intake is associated with increase in inhibitory activity of Tamm-Horsfall protein.
Diuretics like Dicontin–K inhibits the sodium-potassium chloride channel in the ascending limb of loop of henle. It increases the urine output. Calcium channel blockers and α-blockers have been found to be associated with antegrade propulsion of stone by inhibiting ureteral spasm.
Diclofenac sodium inhibits the formation of prostaglandins and helps in relieving pain of stone colic. In addition to anti-inflammatory action, Diclofenac sodium interferes with auto-regulatory response by reducing renal blood flow and does not affects the renal function in normal kidney. Calcium channel blockers are smooth muscle relaxant. Few small prospective studies show that it facilitates spontaneous passage of stone if it is combined with prednisolone which is strong anti-inflammatory drug.
In this study, there was a male preponderance (60%) and median age of presentation was 26.5 years with age varies between 18-75 years. Ureteric stone was more common on right side as compared to left side (60% vs. 40%) in this study.
Most common presentation was ureteric colic in 280 patients (70%), followed by burning micturition in 200(50%) followed by vomiting (40%) and fixed renal pain in 30% cases. Most common sign was haematuria in 290 (80%) followed by urinary tract infection in 230(60%) of patients. Absence of haematuria does not rule out present the stone. According to one study, 67% of patients with ureteric stone had more than 5 RBC per high power field and 89% of patients had more than 0 RBC/hpf on urine microscopic examination.
Total number of patients with stone up to 4mm size were 210(52.5%), 5-6mm were 40(10%) and 7-10mm were 150(37.5%). Patients with stone size up to 4mm were offered regime 1 out of 210 ,120 patients had passed stone with regime 1& 30 patients were referred for surgery because of high grade obstruction they develop. Remaining 60 patients were switch over to regime 2, out of those 48 (80%) patients had passed stone.
Those patients of 5-6mm and 7-10 mm were offered regime 2.out of 190 patients,114 patients had passed stone with success rate of 60%.comparing the efficacy of regime 1 to 2, regime 2 was found to be more effective for upper 1/3rd(P:0.011) and lower 1/3rd (p=0.000). For middle 1/3rd, there was no statistical significant difference was found (p:=0.676).Overall success rate with regime 2 was 80%.
Stone passage rate was highest in the lower ureter 1/3rd (80%) followed by middle 1/3rd (45%) and upper 1/3rd (40%). According to Ueno et al, width is a critical determinant of spontaneous passage of stone. So we considered width as a parameter for patient’s selection. We found that stones measuring 5 mm or smaller in size will usually pass spontaneously in 80% cases, while stones measuring 6mm or larger in size will pass spontaneously in 60% cases.
Though Stone size and location is very important predictor of stone passage, many other factors decide the fate of stone. It is known that the larger the stone lower the probability of spontaneous passage. With regard to the location of stone, our study showed that if a stone was present in the upper 1/3rd of ureter at the time of diagnosis, the overall frequency of spontaneous passage was 40%. The frequency of spontaneous passage of stones in the distal 1/3rd of ureter was significantly higher than that of stones in the upper 1/3rd (80%).
A review of the literature published by Hubner et al in 1993 included 2,704 cases derived from six studies; they reported frequencies of spontaneous passage of 12% for proximal ureteral stones, 22% for mid ureteral stones, and 45% for distal ureteral stones. Review by Singh et al show that medical treatment using either α-blockers or calcium channel blockers improve the stone passage rate for moderately sized distal ureteral stones. Adverse drug reactions were noted in 4% of those taking α-blockers and in 15.2% of those taking calcium channel blockers.
Meta-analysis by Hollingsworth et al also concludes that medical therapy with either calcium channel blockers or α- blockers may increase the chance of spontaneous passage of stone. Steroid has also found to important in the conservative management of ureteric stone. Addition of steroid to α blocker has been found to shorten the time for spontaneous passage.
Overall success rate is 70.5% in this study for stone up to 10 mm in size (282 patients have passed stone out of 400) In our study, higher stone clearance rate was noted with regime 2. Those patients who were not responded to regime-1 were switch over to regime-2 and responded very well (80%). There was a statistically significant difference was noted with regime 2 for at least lower 1/3rd (p=0.000) and upper 1/3rd calculus (p=0.011). Better response rate was probably because of addition of calcium channel blockers and steroids.
Only those patients who required intervention were admitted to the hospital. All other patients were managed at home by medical treatment. No patients in our study showed any significant side effects associated with drugs.
Medical expulsive therapy using calcium channel blocker and steroid is a rational approach for management of ureteric calculi. It is cost effective and patients can be treated on outpatients’ basis. Patients can carry out his day to day work with medical expulsive therapy without significant side effect.


{kind=link}