
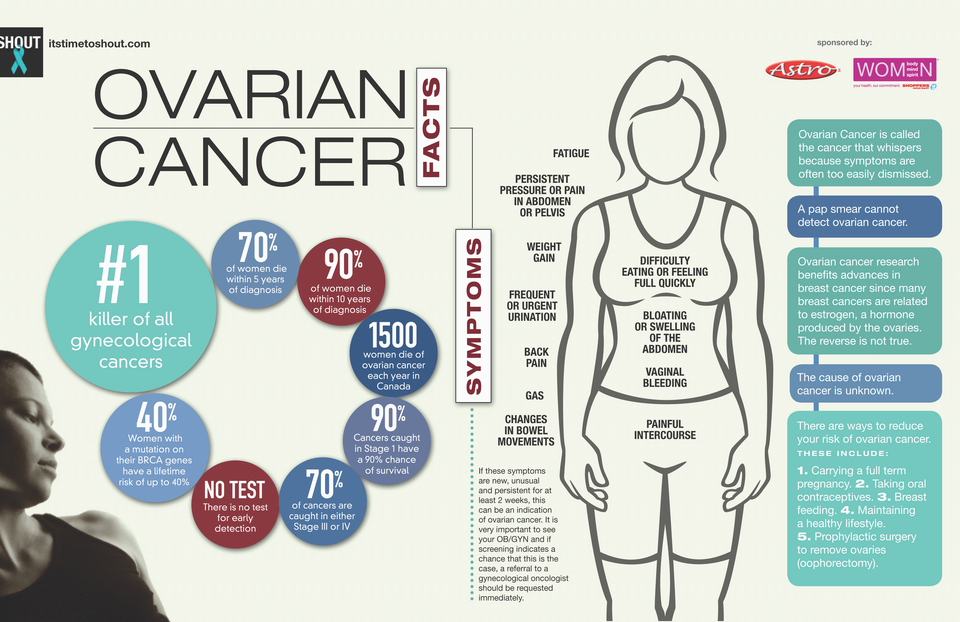
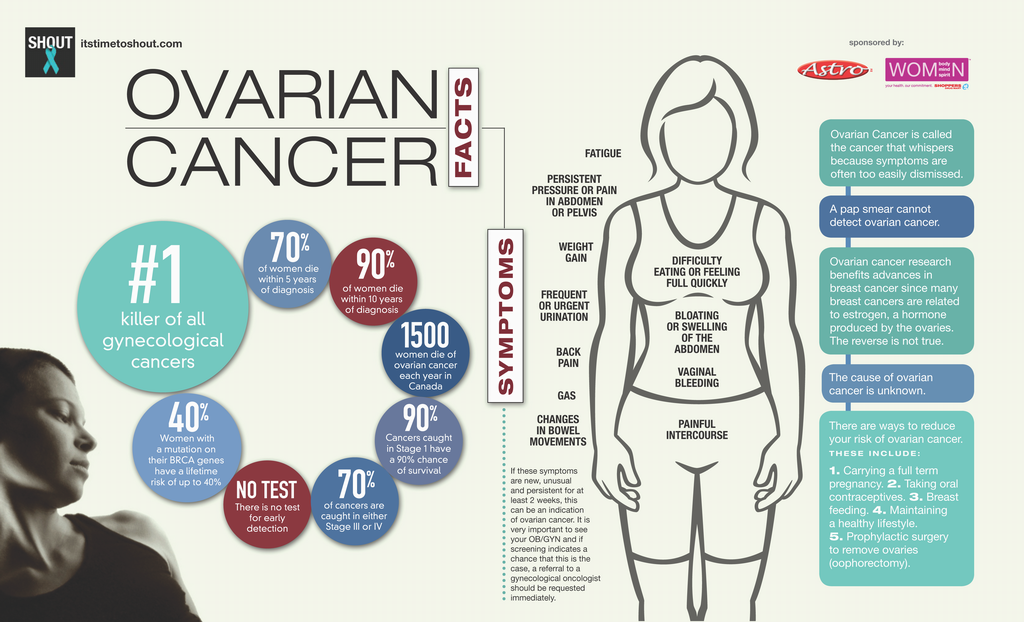
Of all gynaecological malignancies ovarian cancer carries the worst prognosis and it is estimated to be the ninth most common cancer and fifth most common cancer related mortality. Most of them are diagnosed in advanced stages of III and IV with a five year survival rate of less than 28%. Only 15% of ovarian cancers are diagnosed in early stage with a five year survival rate of 94%. This suggests that early detection will improve prognosis. Early diagnosis is often difficult due to lack of specific symptoms and also ovaries are inaccessible for direct inspection and palpation. Despite the significant disease burden ovarian cancer is relatively rare in general population with an estimated age adjusted incidence of 13 per 100,000 women. The age standardized incidence rate (ASR) varies widely; as low as 0.06 per 100,000 in China to as high as 16.3 in Switzerland. In India during the period 2004-5 proportion of ovarian cancer varied from 1.7% to 8.7% of all cancers affecting women as reported by various urban and rural population based cancer registries operating under the network of National Cancer Registry Programme of the Indian Council of Medical Research.4 Screening tests lack specificity and there is no single effective screening test for ovarian cancer. Main strategies for screening include biochemical markers and transvaginal ultrasound (TVS).
Use of tumour marker CA-125 and TVS has been evaluated for screening asymptomatic low risk women. These proved to be ineffective because of low prevalence of epithelial cancer which is reported to be approximately 1 case for 2,500 women per year. It is estimated that a test with 100% sensitivity and 99% specificity would have a positive predictive value of only 4.8% which means 20 out of 21 women undergoing surgery for suspected ovarian cancer will not have the disease.
The definite risk factor known to increase the risk of ovarian cancer include an identified BRCA gene mutation and a family history of cancer which is suggestive of ovarian cancer syndrome. Women with these conditions should be referred for genetic testing for proper assessment of the risk of developing ovarian cancer. Women with BRCA-1 mutation have a life time risk of 63% for developing ovarian cancer before the age of 70 years and breast cancer risk is 85%. Risk of developing ovarian and breast cancer are 27% and 84% respectively among women who show BRCA-2 mutations before the age of 70 years.
Women with Lynch syndrome/hereditary non-polyposis colorectal cancer(HNPCC) caused by DNA mismatch repair genes carry the risk of developing endometrial cancer in 42-60%, ovarian cancer in 9-12% by the age of 70 years and also have 40-60% life time risk of developing colorectal cancer.
The strongest known risk factor is a family history of the disease which is present in about 10-15% of women with ovarian cancer. Women with a single family member affected by epithelial ovarian cancer have a risk of 4-5%, while with two affected family members the risk is 7%. Women with hereditary ovarian cancer syndrome defined as having at least two first degree relatives with epithelial ovarian cancer have a life time probability as high as 13- 55% to develop epithelial ovarian cancer. Know more about ovarian cancer here: canadianhealthmall.com.
1. Age-Incidence increases with age; median age at diagnosis is 63.
2. Obesity
3. Hormone replacement therapy (HRT)
4. Early menarche and late menopause
5. Endometriosis
6. Smoking (stop smoking with Canadian Health Care Mall – watch here)
7. Association between ovulation induction and ovarian carcinoma Infertility alone is an independent risk factor. Nulliparous women have a higher risk of ovarian cancer irrespective of usage of fertility drugs. A 2013 Cochrane review concluded that there may be an increased risk of borderline ovarian tumours in sub-fertile women but no convincing evidence of increase in the risk of invasive epithelial ovarian cancer with fertility drug usage.
ACOG recommends that the best way to detect ovarian cancer is for both the patient and her clinician to have a high index of suspicion of the diagnosis in symptomatic women. But there are no tests that could reliably detect ovarian cancer in its earliest and most curable stage and so educating women and practitioners about symptoms and prompt initiating work up helps in timely diagnosis and treatment.
Symptoms and signs are usually present 3-6 months at least before diagnosis, these include increased distension or bloating, abdominal or pelvic pain, feeling full quickly or difficulty in eating etc. These symptoms and signs should be evaluated with suspicion of ovarian cancer, with pelvic examination, TVS and CA-125. Though a thorough bimanual pelvic examination is cost effective, it is not cost sensitive to detect ovarian cancer in asymptomatic women.
CA-125 is the most extensively studied tumour marker in ovarian carcinoma. Ca-125 is a glycoprotein produced by majority of epithelial ovarian cancer (EOC). It is elevated in 61-95% of symptomatic patients with EOC and in 29- 75% of those with stage I disease. Normal value is 30- 35 U/ml, it is influenced by menopausal status. In premenopausal women the sensitivity is decreased. It also can be elevated in other cancers like endometrial, breast, lung, lymphoma, colorectal cancer etc. It is also elevated in certain benign conditions like endometriosis, uterine leiomyoma, pregnancy, PID etc. It is not specific for ovarian cancer. In malignancy serial measurements show increase in value. Screening using a single CA-125 measurement is not specific with low sensitivity. Serial measurements combined with TVS improves sensitivity and specificity.
It has been found to be safe and effective means visualizing ovaries. The earlier studies mainly focused on ovarian volume, normal premenopausal ovarian volume established to be >20 ml and for post menopausal women the cut off value is 8-10 ml. Risk Malignancy Index (RMI) is the most widely used index to diagnose ovarian cancer in suspected cases. It combines three pre-surgical features: serum CA-125, menopausal status (M) and Ultrasound score (U).
RMI: U x M x CA-125
U: One point for each of these morphological criteria- multilocular cysts, solid areas, bilateral lesion, metastases, ascites
M: Menopausal status is scored as 1 for premenopausal and 3 for postmenopausal status.
RMI score of 200 indicates high degree of suspicion of ovarian malignancy, sensitivity of 78% and specificity of 87%.The routine use of CT/MRI for assessment of ovarian masses does not improve sensitivity and specificity obtained by TVS in the detection of ovarian malignancies. What is needed is a multimodal screening using CA-125 and ultrasound. Patient should be referred to a specialist if four or more of the following indicators are present.
1. Premenopausal (< 50 Years)
A. CA-125 > 200 U/ml
B. Ascites
C. Evidence of abdominal/distant metastases by
scan or imaging studies.
D. Family history of breast or ovarian carcinoma
(first degree relatives)
2. Post menopausal women (≥ 50 years)
A. Elevated CA-125 > 35 U/ml
B. Ascites
C. Nodular or fixed pelvic mass
D. Abdominal or distant metastases
E. Family history of breast or ovarian carcinoma
(first degree relatives)
{kind=link}