


Chronic obstructive pulmonary disease (COPD) is a global public health problem. It is projected that by 2020 it will be the third leading cause of dead worldwide, and the fifth leading cause of years of life lost due to disability coupled with years of life lost due to premature dead (DALYs). The condition affects 10% of the world population above 45 years, and not only 15% of the total smokers but up to 50% of heavy smokers.
The definition provides that, besides being preventable, treatable and characterized by a chronic and persistent airflow limitation (usually progressive), COPD is due to an increased chronic inflammatory response. The pathologic process is initiated by exposure to cigarette smoke or biomass fuels. Exacerbations and many comorbidities that contribute to severity in a particular patient, have an inflammatory nature as well.
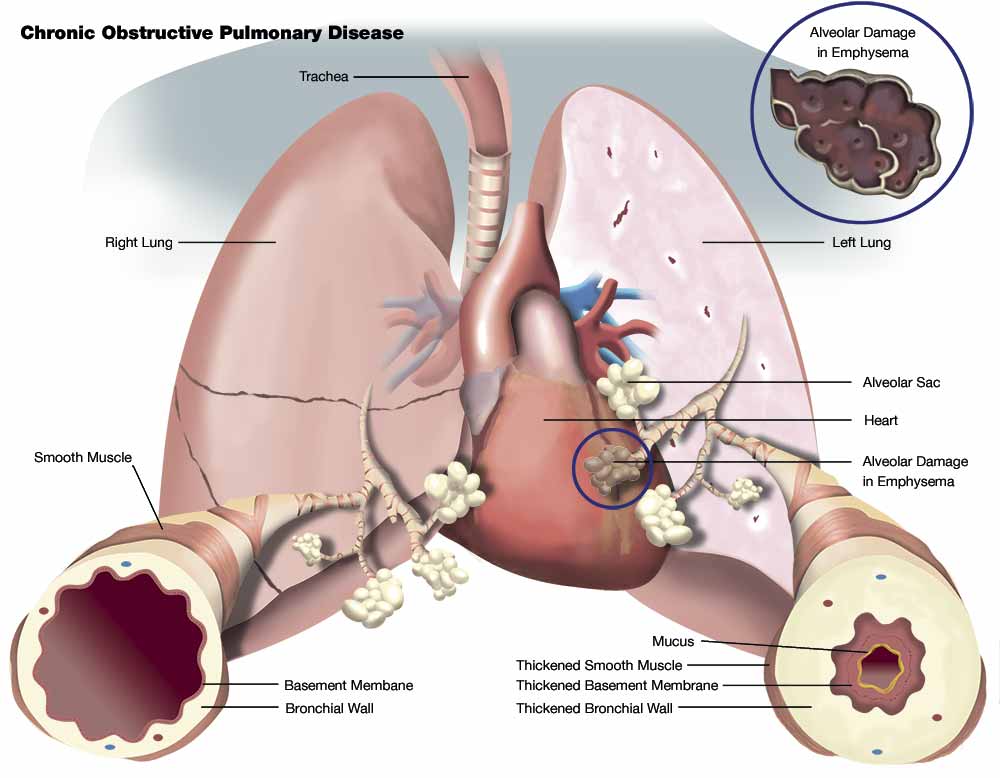
The inflammatory profile in normal smokers is very similar to that of patients with COPD, but less prominent. The concept that emerges is that of an amplified inflammatory response in COPD patients. It is important to understand how the inflammatory response at different anatomical sites causes different physiological sequels, pathological events and clinical manifestations: Central airways (chronic bronchitis), small peripheral airways (obstructive bronchiolitis), lung parenchyma (emphysema), cardiovascular system (pulmonary vascular disease and cor pulmonale) and dysfunction of respiratory and peripheral muscles (systemic disease). The inflammatory process in these compartments is similar, but COPD predominantly affects the small airways and the lung parenchyma.
The aim of this review is to dissect the molecular biology of the inflammatory process and discuss innovative therapeutic strategies for COPD.
Each inhalation of cigarette smoke contains about 10^17 reactive oxygen species (ROS), which initiate the inflammatory response in airways and lung parenchyma. The amplified inflammatory response in COPD is associated with mucus production, proteolysis, fibrosis and cycles of resolution.
The process is possibly determined by genetic factors, latent viruses, oxidative stress and alteration of the Histone Deacetylase-2 (HDAC-2) activity. The type of inflammation that occurs is mediated by the recruitment of different inflammatory cells and the production of distinct mediators, the most important ones will be discussed.
Macrophages are increased in number and activity in the sputum and bronchoalveolar lavage (BAL) of patients with COPD; macrophages play a main role in the inflammatory process. Stimulated by cigarette smoke and other irritants, they release ROS, nitric oxide (NO) and chemokines that attract monocytes, neutrophils and T cells into the inflamed area. Macrophages also have a longer life span, mediated by increased activity of Bc1 -XL anti apoptotic protein.
T cells are CD8 + (suppressor/cytotoxic) subtype Th1/Tc1 (producers of upsilon-interferon) and are located in mucus secreting glands, central and peripheral airways and lung parenchyma. They release granzymes, perforins and tumor necrosis factor alpha (TNF-alpha which induces apoptosis of alveolar type I cells, favoring emphysema.
Neutrophils are increased in the sputum and BAL of patients with COPD. They are attracted by epithelial cells, macrophages and T cells through chemotactic factors; such as interleukin 8 (IL-8), leukotriene B4 (LTB4) and a number of chemokines that belong to the CXC family (cytokines that act over R specific receptors). Neutrophils release serine proteases like Elastase, Cathepsin G, Proteinase-3, Matrix Metalloproteinase-12 (MMP-12) and toxic oxygen radicals, which promote the production of mucus and alveolar destruction.
Is controversial whether eosinophils are elevated in the sputum of stable COPD patients, although they are increased during exacerbation. 10% of COPD patients respond to inhaled glucocorticoids, these patients have a greater number of eosinophils in the airways and greater reversibility to bronchodilators. It has been suggested that this patients may have concomitant asthma. Recently, in a joint effort of GINA and GOLD the term ACOS was developed, as an overlap syndr Asthma and COPD.
Epithelial cells produce TNF-alpha and IL-8 in response to inhaled bronchial irritants. They also generate transforming growth factor beta (TGF-beta) which can cause local fibrosis. Fibroblasts have increased activity and produce extracellular matrix proteins in the small airways (obstructive bronchiolitis). Smooth muscle cells and endothelial cells are also involved in the inflammatory process.
{kind=link}